We’re back with another edition of Fellows’ Case Files! Today, we’re virtually visiting Rutgers University, Robert Wood Johnson Medical School to work through a fascinating pulmonary case. Enjoy, and let us know your thoughts.
Meet Our Guests
Khalil El Gharib completed his residency training at Northwell at Staten Island University Hospital Program and is currently a first year fellow at Rutgers Robert Wood Johnson Medical School.
Sabiha Hussain completed her residency training at Robert Wood Johnson Medical School and her fellowship training at Columbia Presbyterian Medical Center in New York. She is currently a Professor of Medicine and the fellowship Program Director.
Case Presentation
- Patient: 28-year-old male with Asperger’s syndrome and IgA nephropathy.
- Symptoms: 3-month history of progressive dry cough and dyspnea on exertion; later developed mild hemoptysis.
- Notable exposure: Questionable black mold in the patient’s apartment.
Initial Workup and Diagnostic Reasoning
- Vital signs: Hypoxemia (SpO₂ 91% on room air).
- Exam: Inspiratory crackles.
- ABG findings: Elevated A–a gradient (~50), indicating a gas exchange problem.
- Chest X-ray: Bilateral, patchy infiltrates without specific lobar preference.
- Initial management: Discharged with empiric antibiotics for presumed multifocal pneumonia.
Re-Presentation and Further Testing
- Symptoms worsened; now with blood-tinged sputum.
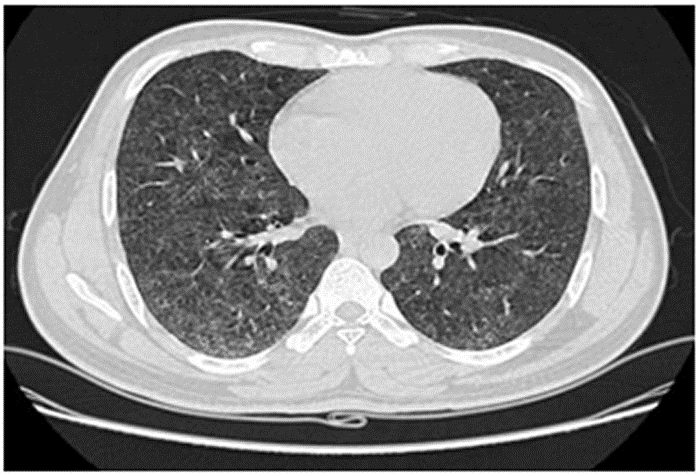
- Chest CT: Showed diffuse ground-glass opacities (GGOs) without fibrosis, consolidation, or lymphadenopathy.
Imaging and Pathology

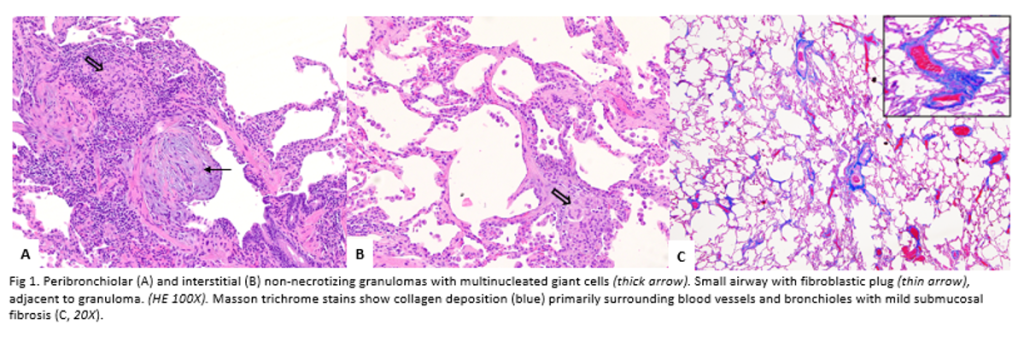
Pathology images a courtesy to Dr Isago Jerrett, pathology resident at RWJMS
Key Learning Points
Diagnostic Fram
Episode Transcript
Hey, everybody. Thanks for tuning in to Palm
Peeps. We are very excited today to be
joining you with another episode. We haven't done
one of these in a little while. We're
getting a preliminary
fellows case file today. These are one of
our favorite
episode types that Monty and I get to
record and meet fellows and program directors from
across the country. So we're very excited to
be back with you and take you through
(00:38):
a really interesting case. But before we do
that, as always, join with my partner in
crime, Christina Montanor. Christina, how's it going?
Hey, Ferb. Good morning. Doing great. Glad to
be back with you. I feel, like, haven't
seen you in a few weeks, so this
is always the best part of my week.
So excited to be back. And as you
said with another Fellow's case files, I feel
like we've had some new initiatives for 2025
(01:00):
including our guideline series, which have been fantastic.
But the Fellow's case files remain one of
my favorite episodes that we do because we
get to hear from fantastic
educators, trainees from across the country. So
really excited today to be virtually visiting Rutgers
University and Robert Wood Johnson Medical School, which
I have not visited personally, but I still
(01:20):
think for if we're gonna go on a
summer road trip in a bus and Yeah.
Visit all the Fellowes case files that we've
done. So I still think we're gonna make
that happen. A %. A bus or Winnebago,
we'll have to we'll have to decide on
the best mode of transport for us.
Exactly.
But really excited to get started today, and
we have two guests today, and I have
the honor of introducing our first guest. We
(01:42):
have doctor Khalil Elgarib.
Khalil completed his residency training at Northwell at
Staten Island University Hospital program and is currently
a first year fellow at Rutgers Robert Wood
Johnson Medical School. And Khalil reached out to
us with a fantastic case that I'm really
excited for us to go through today and
such an honor to have you on the
show today. Welcome to Palm Peeps, Khalil.
(02:03):
Thank you for the introduction, Christina. I'm a
big fan of the show and I'm thrilled
to be here.
Yeah. Thank you. We're thrilled to have you,
and thanks for listening, certainly.
Next, we have doctor Sabia Hussain. Sabia completed
her residency training at Robert Wood Johnson Medical
School and her fellowship training in pulmonary and
critical care at Columbia Presbyterian Medical Center in
New York, where I did my fellowship. So
(02:25):
we're bonded for life by that. She is
currently a professor of medicine, and the program
director for the pulmonary critical care medicine fellowship
program. Thanks for coming on the show.
Oh, thanks so much for having me. I'm
really excited.
Wonderful. Excited to have you and walk through
some really great teaching points with us today.
As our quick disclaimer, just a reminder, the
(02:46):
podcast is not meant to be used for
medical advice, and the views we expressed today
do not reflect the opinions or policies of
our respective employers.
The case we'll present today is HIPAA compliant,
and some details might have been changed to
protect the privacy of our patient.
But let's go ahead and dive into the
case. Khalil, you as I said, you this
was your brainstorming
(03:06):
and great
educational feature that you wanted to share on
the show today. So why don't you go
ahead and tell us about the patient that
you met and how they initially presented?
This is a patient that we met a
couple of years ago in the clinic. It's
a 28 year old male patient with a
past medical history of Asperger's syndrome and IgA
nephropathy
who presents to the emergency department for shortness
(03:28):
of breath and cough. The caregiver reports that
the patient has been having dry cough and
dyspnea ambulation,
progressing for the past three months prior to
the presentation to the ED.
The patient didn't have any wheezing, no chest
pain, no palpitations, or any constitutional symptoms.
The patient's medications were van stropin and oxcarbazepine,
(03:49):
and his social history is mainly notable for
questionable
black mold exposure in the apartment where he
resides.
Great. So thanks so much for sharing that,
Felil. And I say fairly common pulmonary visit,
at least from a complaint standpoint and chief
complaint that we're hearing, although in a much
(04:09):
typically younger patient than we probably see on
average.
So, Dave, I would love for you to
share how you'd start your diagnostic reasoning approach
for the specific patient.
Yeah. Absolutely. This is something we've talked about
a lot on the show about critical thinking
and diagnostic reasoning. I think we
everybody uses
variety of modalities to think about a new
(04:32):
patient, and it's important to have some metacognition
about that. And so I think the common
ones that people use are diagnostic schemas and
illness scripts. You hear about some symptoms. You're
trying to fit them into a pattern that
you recognize,
and then you're trying to go down based
on different likelihoods,
different parts of that sort of flow diagram.
And thinking about that consciously is that sort
(04:53):
of type two slow thinking. We do it
very unconsciously while we're gathering information in the
clinic, that sort of type one rapid reasoning
response.
And this is a very common complaint. As
you said, we're thinking about a patient who's
coming in with cough, and then we wanna
amend just that
basic presentation
with some info that will change the likelihoods
of diagnosis. So those have to do with
(05:15):
the chief complaint, the substrate, predisposing
conditions, and exposures. As you said, this is
a relatively younger patient. We don't have any
history of smoking or things like that lead
us down a different pathway, and we're thinking
about
what sounds like a progressive chronic dry cough.
And so if we were thinking about that,
the most common reasons for that in The
United States are GERD, postnasal
(05:36):
drip, cough variant asthma. There's actually an excellent
review article that just came out in the
New England Journal on chronic refractory cough. It
was a really great read and definitely good
for any pulmonary provider or fellow to read
about.
But I think the key thing that helps
me distinguish how I'm gonna approach this patient
is that he's also having dyspnea on exertion.
Exertion. And so cough in isolation
(05:58):
and a dry cough in isolation
is very different than a cough with dyspnea
on exertion because now I'm starting to think
a little bit more about the lung parenchyma,
about airways disease that's reaching a level that's
affecting the patient's ability to exert themselves. I'm
starting to really think about if that cough
is reflecting
some more progressive pulmonary process.
(06:18):
And then one thing of interest that the
patient brought up, and this is not uncommon,
is that they talked about a possible exposure
to mold. And so I think mold is
a broad bucket term, hot term for most
people, like in the public. And so you'll
often get a patient that comes up and
says, I was told I have mold or
there's mold in the workplace, and they're a
little bit worried about that. And it certainly
should affect our thinking some. So, Sabi, I
(06:40):
was wondering if you could tell us how
you think about your diagnostic reasoning and what
changes about it when a patient mentions a
mold exposure.
Yeah. Thanks so much, Dave. Yeah. I think
that there's a lot of things that when
you have a patient that comes in that's
having progressive
symptoms and dyspnea,
especially as you were saying, this younger age
(07:00):
population, you really do have to think about,
like, exposure.
And and so this individual tells you a
little bit about mold and mold exposure. So
that's like
puts your thinking caps on and figuring out,
like, what does this mean? And as mold
is, like, all around us, it's ubiquitous. It's
in the indoor and the outdoor environment.
And in majority of cases, most humans
(07:23):
and and mold coexist. Like, they don't have
any issues or problems
that are going on. But then there are
individuals
that this mold could then re lead to
other things like allergic rhinitis,
complications
of allergic
asthma. And then less frequently, these moles can
result in atopic conditions
(07:45):
such as allergic bronchopulmonary,
astragelosis,
and allergic fungal
rhinosinusitis.
Rarely do they present as, maybe in this
instance,
as hypersensitivity
pneumonitis, and that really would be something that's
high semi differential right now in this individual.
And so
(08:05):
you think about, like, exposures. So sometimes, like,
occupational
exposure that can cause these kinds of hypersensitivity
and pneumonitis symptoms.
And so we do
try to figure out exactly
how much exposure that individual is happening is
having.
Is that exposure
(08:26):
continuing?
And all those kinds of things does go
into,
will we take this mold exposure seriously?
That's really great. Hey. I think you bring
up some great points so that we have
to think about this. It puts it at
the forefront of our mind. That being said,
most of the time, these things are mild
(08:47):
exposures, and there might be something else going
on, so we don't just hone in on
that. And then I think you also hit
the nail ahead of figuring out
how significant and real and continuous this exposure
is. Is this something the person can get
away from? And there are a variety of
different ways to do that, including having somebody
even go out to a patient's work or
home to try to understand what's going on.
(09:08):
So these are things we'll have in the
back of our head as we continue to
hear more about the patient. So, Kahlil, can
you move us forward in case? Tell us
a little bit about the patient's exam.
Sure. In the EDE, the patient was hemodynamically
stable, but his pulse ox was around 91%
on room air.
His, examination was mainly notable for crackles in
the right upper and lower lung fields as
(09:29):
well as in the left upper lung fields.
So, Christina, can you tell us how this
exam would influence your thinking?
Sure. Thanks so much, Khalil. I think here,
it's really important, the pulse ox that you
mentioned as well as the physical exam findings.
So I'd like to go ahead and first
talk about the ninety one percent on room
air. Right? This is atypical for a 28
(09:49):
year old at rest, Something that I would
consider to be abnormal and would really probably
have our head head scratching. Something's going on
here. I think we'll definitely wanna get a
gas, and this would be a patient who's
has,
be I would be concerned about having exertional
hypoxemia.
So if we were able to get an
ambulatory sat on him, this would be a
patient that I would definitely consider that in.
(10:11):
But really starting to think about
with this 91% on room air honing in
on the diagnosis and the etiologies of hypoxemia.
So I think with that
adding to that are is a physical exam
finding. So you said there's crackles scattered throughout.
And while we say sometimes you can say
dry versus wet crackles, the physical exam, I
(10:31):
think, is somewhat not the best at distinguishing
between those two etiologies.
Well, I think using our exam, knowing an
abnormality,
trying to figure out what diagnostic test would
be appropriate to order and what we anticipate
to show on that diagnostic test. But I
think when we're really saying, like, we we
feel like we hear a wet crackle, I
tend to correlate that with more of an
alveolar filling process,
(10:53):
whereas I hear, like, dry or fine crackles
or even, like, the Velcro
crackles, sometimes that's commonly used for terminology,
I would correlate that more with a pringable
process.
So I think either one is definitely concerning
in this patient and lines up with the
relative hypoxemia that we're seeing. And I think
to think about because you think as we're
seeing someone very early on in the course,
(11:14):
there's gonna be a lot of tests that
are ordered, but this is a patient, and
when I work with trainees, would really like
to say, based off our physical exam and
based off the current diagnostic testing that we
have, like, what do we anticipate we're going
to find on x diagnostic test? As opposed
to say, let's wait to see what the
CT shows. It's based off this. I think
the CT show is going to show
(11:36):
either alveolar filling process
here. I if we were to get PFTs
on this patient who has a pulse ox
at 91% on room air at rest, we'd
probably be concerned that there's some diffusion capacity,
so probably an impairment in DLCO.
So just another way to start to frame
what diagnostic test we wanna select and what
we anticipate to see based off the limited
but great data that you've presented so far.
(11:58):
And I'm sure this patient did have some
additional workup done. So, Khalil, any did the
patient get a an ABG in any other
labs that you wanna share at this time?
Yeah. Of course. So the patient the labs
were ordered, including a CBC with DIF and
a complete metabolic profile.
TMP and the CBC was with were with
the normal limits, but an ABG on Lumiere
(12:20):
was mainly notable for a pH of 7.38,
a p c o two of 34, a
p o two of 55, and a bicarbonate
level on the metabolic profile that was of
20.
Thanks, Khalil. This is super helpful. As Christina
was mentioning, we are thinking about etiologies of
hypoxemia now interestingly because he's not hypoxemic
(12:41):
by standard criteria, but I think we all
know that twenty one percent ninety one percent
for a 28 year old in room air
would be abnormal.
And this gives us that same indication. The
PO two is 55. It lines up pretty
nicely with us. And so my first sort
of step on this is if you have
a patient, they have shortness of breath, is
to calculate an AA gradient. And this is
(13:01):
a perfect patient to do that in. They're
not that sick where a lot of the
factors are gonna be changing in the AA
gradient. They're on room air, and they're a
young patient where we have good expected normal
values. And I think all of everyone will
reach back and remember their equation, but f
I o two times atmospheric pressure minus water
pressure, which in our standard, we can simplify
down to one fifty minus p c o
(13:22):
two over 0.8.
That is giving us our sort of metabolic
ratio and profile. And that gives us an
estimation of their alveolar oxygen content. And then
we're subtracting
from that, our p a o two. And
for this patient, we get a gradient of
50, which is certainly well above the normal
expected for someone who's this age, which would
be in the 10 to 20 range.
(13:43):
And so now we have hypoxemia. We have
hypoxemia at rest. And so we could do
other things like giving oxygen, trying to see
how that changes. But we are really starting
to worry here now about a BQ mismatch
or sort of shunt situation. DLCO obviously can
do this as well, but it very unusual
for a 28 year old to have relative
hypoxemia and the elevated gradient at rest, just
(14:06):
from DLCO. We'd really think about exertion as
driving that. And then because you gave us
a metabolic profile, we can also think about
the acid base status. We see in this
that there's a little bit of a metabolic
acidosis with some respiratory compensation. So that's just
something for us to think about as we're
gonna keep approaching this patient. So now our
our differential that had started as that dry
(14:26):
cough, then maybe dry cough or dyspnea, is
now a little bit more focused on hypoxemia
and crackles. And so we can assume that
we're gonna explain those other findings by explaining
this one and kinda move forward the case
from that.
So based on the abnormal exam, based on
that abnormal gas exchange, I'm sure that this
patient is going to get some imaging. So
we will post all the images from this
(14:47):
case so everybody can follow along and review.
But, Cleo, maybe you can walk us through
the imaging studies.
Yeah. They did a chest x-ray on this
patient in the ED, which showed patchy bilateral
infiltrates without any specific regional or lower predilection.
There were no associated mediastinal abnormalities or any
pleural effusions.
(15:09):
So these opacities seem not to be interstitial,
but seem to be to represent actually airspace
disease. The list of differential diagnosis that the
EDI attendings were thinking of seems to be
broad, but at least we can narrow it
down to alveolar processes rather than interstitial ones.
Among the more common alveolar etologies is pneumonia,
might be multifocal in this case, but can
(15:30):
also include aspiration, tuberculosis,
sarcoidosis,
certain types of cancers, either primary, pulmonary, or
metastatic disease to the lung. So, again, we
have various differentials that we might be thinking
of in front of this clinical case.
Thanks, Kaleo. And I think those are really
great differentials
to think about. Right? And probably an exercise
(15:53):
that you could do is list the differentials,
and then as you get more aliquots of
information,
you can move those differentials up and down
based off the data and kind of the
pretest probability.
So I agree. I think that the differential
for this patient is still broad. We're still
keeping in mind this potential mold exposure.
And probably some of these that you said,
an ammonia process, if this has been more
(16:14):
of a subacute
three month process going on, like, I that
can't completely rule that out, but would probably
start to put some rearrange those in certain
instances just to to see. So I would
probably move infectious down lower on my list
of differentials.
But great ones great differentials that that we
have so far. And love for you to
tell us and walk us through what happened
(16:35):
next for this patient.
As you mentioned, infectious etiologies of the presentation
might be less probable, but the ED physicians
mainly addressed it as a possible multifocal community
acquired pneumonia.
And since the patient has a good social
support, mainly his mother at home, he was
discharged on empiric antibiotics with an outpatient pulmonary
(16:56):
clinic follow-up in a week.
However, the patient presented to the ED five
days later with worsening symptoms and with a
cough that has now a blood tinged sputum.
Thanks so much, Cliff, for taking this through.
Yeah. I think that that your explanation is
really right that maybe we have some signs
of not being quite sure of infection. That
being said, we do this all the time.
(17:17):
Like, if common things being common, we have
to still consider it, and
the low risk of an antibiotic course plays
in. But this is an important thing that
comes up as what are we calling community
acquired pneumonia? What when are we starting to
put on our hat to think about some
other things? Seems like he still has something
lingering, could have some superimposed infection at this
point. But, Sabia, I was hoping you could
(17:38):
walk us through CAP. We see and we
treat really often, but there's always this range
of certainty. Sometimes it's super obvious, and sometimes
it's a little subtle. And just hoping you
can talk us through how you think about
this diagnosis and what do you think about
it relative to this case?
Yeah. Thanks so much. Yeah. I think that
Kalia was really right on in terms
of you know, in fact, your CDology seems
(18:00):
a little bit less
likely, but I mean, being
in the ER with all these patients that
come through, I don't blame them for saying,
okay. Maybe you have something superimposed right now.
Let's make sure we take care of this,
and then we'll see. But most of the
time when you're talking about, like, a community
acquired pneumonia,
we really,
you have to have a constellation of symptoms
(18:21):
like fevers,
along with the shortness of breath, maybe having
x-ray findings as so as, like, an alobar
consolidation.
Although you can have these alveolar kind of
infiltrates that can give you this picture of
multifocal pneumonia.
Atypical pneumonia is all those kinds of things,
and there's ground glass opacities that can happen.
(18:42):
And then oftentimes, you give them antibiotics, and
then the pneumonia resolves. In this instance, it
didn't seem that's what happened is this person
comes back to the emergency room with ongoing
symptoms. And in patients who have who are
immunocompromised,
it's really important to give them
antibiotics. And I don't know how much of
this he does have, like, an IgA
(19:03):
kind of nephropathy.
Does this make him somewhat much more symptom
much more likely to have atypical kind of
presentation?
And so something to think about in this
instance.
Totally. And I I think the the we
talked a lot about the diagnostic process. I
like to kinda show flow diagrams, but then
also say the flow diagrams are still just
(19:24):
a probability. Right? And you always have to
factor in the prevalence in the population.
But then we sometimes don't always do the
same really rigorous thought process, the treatment process.
And so it may just be worth having
some treatment to take a question off the
table, especially if that treatment is low risk
tolerated short in duration. And as you say,
(19:44):
when you see sort of these types of
cases in the emergency department, I think with
an infiltrate on imaging and some hypoxemia
is maybe the better part of valor to
even try to treat it and see what
happens. And then take your next steps from
there. Yeah. And especially because he's, like, relatively
young.
So you're you're like, sweating your eyes. I
think that if he was older, it will
be a very different kind of process. Yeah.
(20:07):
Or immunocompromised,
like you indicated. Yeah. It might change things
a little bit as well.
Yeah. Totally agree. So, Kahlil, when this patient
came back then with worsening symptoms,
right, I think this, as I maybe talked
about earlier, alluded to, just you have the
ability
to reassess and renew your diagnostic differential in
the diagnostic process.
(20:28):
So I'd love for you to walk us
through what happened next and what were the
initial thoughts on his representation.
Yeah. They reassessed the patient in the ED,
and they repeated an x-ray. It showed a
similar appearance to the one done on the
first presentation a couple of days prior.
And for to advance in the diagnostic process,
a CT scan of the chest was done,
(20:49):
which showed diffuse ground glass opacities
with, again, no specific location predilection, no consolidation,
no mediastinal or hyaloid lymphadenopathy,
and there was no pleural disease.
Great. And I think I think the CT
scan is definitely
helpful and indicated in here. And and I'd
(21:09):
love and I know in a minute you'll
talk us through a little bit more of
the diagnostic reasoning. But before this, I wanted
to just resummarize the case because I think
this is gonna be a case that you
will continue to see throughout the remainder of
your fellowship and probably a case that a
lot of our listeners today have had the
opportunity to treat and work up as well.
But just to briefly summarize,
(21:30):
young man with a past medical history notable
for Asperger's and social history notable for mold
exposure,
who's presenting with chronic worse who sorry. Who's
presenting with a
chronic worsening cough and dyspnea, now progressing to
small volume hemoptysis,
who's found to have relative hypoxemia
on room air with an elevate
with an elevated AA gradient
(21:51):
and scattered GGO nodules on CT scan. So,
Kahlil, could you share with our listeners how
you would approach this diagnostically?
Thank you, Christina, for the summary. So at
this point, our diagnostic process will be based
on the findings of the CAT scan and
the temporality of the symptoms.
Having ground glass opacities means that the process
(22:12):
is most likely to be alveolar.
Again, differentials remain broad, but the underlying cause
seems to be a subacute one that tends
to be chronic.
Infectious etiologies are less likely in front of
this alveolitis.
And in the setting of exposure to black
mold, hypersensitivity pneumonitis
like doctor Sabia, doctor Hassan actually mentioned, was
high on offered on our different differential.
(22:33):
At this point, blood and sputum cultures returned
negative, and we decided to proceed with the
diagnostic bronchoscopy and the BAL.
We performed the BD bronchoscopy,
and the fluid that came back was turbid,
and cell count was about 9,000, predominantly neutrophilic.
Later on, AFB, respiratory,
and fungal cultures came back negative.
(22:55):
We also performed a hypersensitivity
pneumonitis panel that came back positive for high
titers of antibodies
against,
and be patient with me over here, Oreobacidium
pululans, which is a fungus
frequently found in black mold.
Patient. That was perfect. I'm glad I don't
have to try to pronounce that.
But this is great. I love the way
(23:16):
that you're approaching this case. We seem to
have a patient that had a few things
that could be pointing towards hypersensitivity pneumonitis, and
so we're gonna be aggressive in that workup.
And so I think sending the lab panel
to adjust our pretest probability is gonna be
really helpful. I also think, like, a bronchoscopy
at this point just makes a lot of
sense. Right? Patients come back, failed one course
of antibiotics,
(23:37):
gram last opacity, small volume hemoptysis.
You could think about trying to do other
empiric treatments, but we just have to know
what's going on. And bronchoscopy with cell count,
interestingly,
is part of getting cultures really helpful for
ruling out infections and especially helps us with
atypical infections. Like, we're gonna set it AFP.
We're gonna have a broader respiratory panel.
(23:58):
But, cell count itself can be in the
workup of some of our interstitial lung diseases
and our hypersensitivity
pneumonitis as well. Okay. So this patient now,
we have a bunch of things that are
pointing towards hypersensitivity.
We have a presentation that's consistent, subacute to
chronic, progressive, cough, and hypoxemia.
We have ground glass opacities on the CAT
scan, and we'll post it for you all
(24:19):
to see, but with features that may think
of make us think about hypersensitivity
and pneumonitis.
To say some of these explicitly, I think
we'll talk about it, but there are different
patterns we can see. We can see more
upper lobe distributions and hypersensitivity pneumonitis. We can
see more air trapping and things like that
in association with our ground load,
our GGOs.
We also have a known mold exposure by
(24:40):
history,
and this is now also confirmed based on
an antibody profile. So obviously this is raising
it really high.
There are some things that are not quite
classic. The B a L B and PMN
predominant is not what we classically read about.
We really think about lymphocyte predominant in the,
in the HP process. So we'll just take
those things into consideration.
(25:01):
So clearly you are taking care of this
patient, your fellow, I'm sure, very industrious about
reading about all of these possibilities.
So can you tell us a little bit
more about the diagnosis of HP and how
one comes to that diagnosis?
Sure. Let me start first with a quick
definition.
Hypersensitivity
pneumonitis is a complex ILD caused by exposure
to an inhaled antigen
(25:21):
with many phases, extending from self limiting disease
to relapsing or progressive inflammatory disease to chronic
fibrotic disease resembling IPF.
We categorize patients now as having nonfibrotic or
fibrotic HP. We used to say that patients
might be having acute versus subacute versus chronic
HP, but we were forgetting about this definition.
(25:43):
And the high resolution CT scan of the
chest plays a key role here in the
diagnostic process.
Early disease manifests with ground glass nodules distributed
across all lung zones.
This inflammation leads to small airway narrowing, causing
lobular air trapping.
Sometimes this process might create what we call
a three density pattern, which is a combination
(26:03):
of normal appearing globules,
ground class opacities, and globules of decreased density
and vessel size.
And this CT pattern is highly specific to
HP.
Later in the process, signs of fibrosis might
appear, combining reticular abnormalities, traction bronchiectasis,
loss of lobular volume, and honeycombing.
(26:24):
PFTs, if performed, would show a restrictive pattern,
and the BAL is usually done on these
patients.
Cell count would show high WBC count like
you mentioned, Dave, but differential might be mixed.
It might be neutrophilic
or lymphocytic predominant and tends to be lymphocytic
predominant actually in later stages.
Other work of that what we might be
(26:44):
doing is specific serum IgG tests that can
be valuable to pursue suspicious exposures or point
toward an as yet undetected exposure.
But there is a lack of well defined
predicted values for specific IgGs, and the tests
cannot really differentiate between sensitization
and disease.
So it is mainly a combination of suggestive
(27:04):
history and exposures,
imaging features, and some labs that would lead
us toward a diagnosis of HP.
Thanks so much, Khalil. That was just a
great summary
of what learners should expect when they're thinking
about this in
imaging and history findings that are so important.
And I think such a great teaching pearl
that you also included was really this new
(27:27):
terminology
used to classify hypersensitivity pneumonitis, which is now
nonfibrotic or fibrotic.
So glad that you brought that up. And
for you in training and for others listening
today, can I can now have that framework
as well?
So coming wanna come back to our case,
though. So did you feel that at this
point that this was a a concrete diagnosis?
Were you a % confident on it? Or
(27:49):
were there any other diagnostics that you and
or the team felt needed to be pursued?
Mhmm.
So there was still an uncertainty regarding the
diagnosis of HB in this case.
We opted then to pursue a long biopsy
via VATS, and a sampling of the middle
and right lower lobes showed small airways with
mild chronic inflammation of the epithelium and submucosa,
(28:11):
occasional entraepithelial
eosinophils and neutrophils,
mild smooth muscle hypertrophy, and mild submucosal fibrosis.
Also, on the pathology, there were several poorly
formed non necrotizing granulomas and occasional giant multinucleated
cells adjacent to the small airways, as well
as in the interstitium.
(28:34):
Thanks, Cleo. And I'm sure, in this case,
right, I think the decision to do some
of these more advanced diagnostics, right, the bronchoscopy,
the vats, probably having a multidisciplinary
team, a lot of people probably thinking about
what makes sense for this patient. So thank
you thank you for sharing that, and thank
you for sharing the the pathology
as well. I and I think that this
is gonna be important for trainees. I feel
(28:55):
like some of this is gonna be it's
kinda like board questions that you're writing for
yourself, Khalil, in the future and for those
listening. But there are a number of things
on the biopsy that make the diagnosis
of HP more likely. A couple things that
you mentioned, right, the small airway diseases with
some air trapping on a background of mild
chronic
inflammation is really gets my attention. There's also
(29:16):
some non nepotizing,
as you said, poorly formed granulomas,
some giant cells, and mononuclear
infiltrates.
And there are multiple pulmonary diseases that can
have granulomas,
though, so it is important for us to
think about what process
is here, which other disease manifestations that we
can eliminate, and those that are gonna still
(29:36):
remain at the high highest on our differential.
So, Sabija, I'm wondering if you can share
with us how you think about granulomas on
a lung biopsy.
Yeah. Thanks so much, Christina.
Granulomas is sometimes the bane of our existence,
but we actually often get CAT scans that
have these tiny little nodules that come back
as granulomas.
What does it mean? And so I think
(29:57):
this is a great case to go through
some of that,
as most granulomas are caused by infectious etiologies,
either fungal or mycobacterium.
And remember when you do have granulomas
that you do have to make sure that
those are ruled out. So you have to
make sure that those stains are done, the
AFB stains, and then fungal skin stains are
done, and those are negative, and that you're
(30:19):
watching out for those cultures, which may take
time. So it may take six weeks until
those cultures have come back to definitively say
that this is a noninfectious
etiology.
And so you have your infectious,
as I said, your mycobacterium as well as
your fungal, then then you have your noninfectious
etiologies
of granulomatous
diseases
such as Wegenerous, granulomatosis,
(30:40):
the hypersensitivity pneumonitis that we're entertaining in this
instance,
hot tub, lung disease, as well as aspiration
pneumonia.
Sarcoid is also something that we look at.
Remember, sarcoidosis
is a disease of exclusion,
meaning that you have to exclude every other
ideology before you say this person has sarcoid.
Now one of the things that you guys
(31:00):
were talking about was like this, how do
the granulomas
look like? Are they tight? Are they loose?
What's going on? And that really does help
you differentiate between
different
ideologies.
So when you're having, like, loosely formed granulomas
in the background where you're having these inflammatory
infectious
inflammatory processes,
(31:21):
you're gonna think more along the lines
of hypersensitivity
pneumonitis. Whereas
if you're having really nice tight granulomas, then
you're thinking more along the lines of sarcoid
as something
as the ideology of your patients underlying lung
disease.
So remember that hypersensitivity
pneumonitis has this triad of findings that we
(31:44):
all have been going through a little bit
of. These poorly formed granulomas,
and you're having this
inflammatory and then also multilucleated
giant cells
as part of your pathological
findings.
Thank you for walking through that for us.
I think this is as you said, sometimes
granulomas or biopsy results can be confusing for
(32:06):
us. And and the presence of granuloma is
great because we have something we have to
act upon, but it can be difficult at
times to
to delve through. And so it's really helpful
to have a framework. As you indicated with
this sort of triad for HP, the pathologist
can often say this is very likely to
be HP, but that's not always the case.
We often think of
biopsy and pathology as the goldest of gold
(32:28):
standards in medicine, and it definitely is. I'm
not I think it's always so helpful to
have the information.
But often the pathologist can just tell you
what they see, and that doesn't always tell
you what the diagnosis is. Like you said,
no pathologist is going to write this is
sarcoid based on this biopsy,
but if they have these non necrotizing granulomas
and big mediastinal lymphadenopathy
(32:48):
and they're the right demographic and everything else
has been ruled out, we know that helps
make us a diagnosis. So it's really helpful
to look at slides, read through reports, and
then think about how we integrate that knowledge
into making a final diagnosis for our patient.
So with all of that and our high
pretest probability by the time of biopsy and
then our consistent biopsy results, seems like we
(33:09):
have a good solid diagnosis of HP for
this patient. We are gonna do a whole
episode on the treatment of HP coming up,
so I don't wanna
dive too much into it, but I do
wanna hear a little bit about and the
wrap up of our case. So, Kahlil, can
you tell us about the basic tenants of
treatment for HP and how this patient was
treated and responded?
Sure. The mainstay of treatment is antigen avoidance
(33:31):
and removal of the offending agents.
Steroid therapy is debatable in the management of
HP, but has been used in severe cases.
Here, the patient switched apartments,
so supposedly, he's no longer exposed to mold.
And we also started him on prednisone forty
milligram every day for a month with a
slow taper over the next six months.
Patient improved symptomatically,
(33:53):
and the HS x-ray done six months after
we first saw him showed resolution of the
previously described infiltrates.
That's awesome. Delgrad, he responded. And I cannot
stress enough the importance of antigen avoidance. This
is not always possible, but it's very difficult
to treat a patient if they can't change
their exposure at all, even with medications, just
because they already have this underlying and then
(34:15):
continuous process going on.
This is a really amazing case. We're very
excited we got to do another fellow's case
files, and we thank you guys both for
being here. We love building this network and
getting to know trainees and program directors across
the country, and we're excited to induct Rutgers
University and Robert Wood Johnson Medical Center into
that network. And so we'd love for each
of you just to highlight what you love
(34:36):
about being there, but about your education and
about the program, and we're all ears. So,
Kilo, why don't we start with you?
So what I really like about my training
here at Rutgers Robert Wood Johnson Medical School
is the supervised autonomy that I get. Also,
we do encounter a lot of complex cases
inside the ICU that we have to manage.
(34:56):
Even if we have to manage them autonomously
inside the ICU, as well as the diversity
of cases that we encounter in the pulmonary
clinic. Yeah. We're seeing the best of both
worlds, if I would say, in the outpatient
clopidmonary clinic and the inpatient
ICU setting.
That's great. That's wonderful.
Flavia, anything to add?
(35:18):
Yeah. Echo what Khalil was saying. It's really
fun being at Rutgers. I know we're, like,
between New York City and and Philadelphia, so
we get a lot of diverse cases here.
And it's really fun to teach in this
environment, and Rutgers seems like it's, like, taking
over the entire state.
So I think that in that kind
(35:40):
of environment, we get a lot of very
diverse case case loads. We actually recently had
the the Mexican consulate next door, so we're
getting a lot of it was from throughout
the world, like this hot bodge of individuals.
So we get a lot of different disease
processes.
Wow. That's really interesting. Yeah. The people in
New Jersey, thank you for their extensive network
(36:01):
that's being built. I'm sure.
I know. That sounds fantastic. Sounds like a,
yeah, training program with really diverse patient care,
fantastic education, and what seems like a really
supportive environment. So glad to have you on.
And for those listening today, think of this
as a potential future fellowship home for you.
And as we end our case today, I
(36:22):
know we like to wrap up each case
with a takeaway point.
I think mine today is I'm just gonna
say relisten to Khalil talk about and define
HP,
but I really like to get how you
mentioned we're moving towards this fibrotic, non fibrotic
characterization
of hypersensitivity
pneumonitis.
And I think you also mentioned the triple
density sign, which can sometimes be seen with
(36:44):
with HP.
So just making sure learners remember that and
can their diagnosis and, clinical reasoning when looking
at a patient together. Farf, what about you?
Yeah. Yeah. I think we have a radiology
rounds on the triple density side. We'll repost
it so people can take a look.
I'll build on that. I think Khalil mentioned
something that's really helpful to consider is that
(37:05):
there's this
acute to chronic,
non fibrotic to fibrotic spectrum of HP, and
some of the classic features we think about
are really more in that chronic HP populations.
That BAL lymphocytic predominant
is a lot from the ILD literature, maybe
a more chronic population, maybe some more fibrosis,
but can have a neutrophil predominance early on
(37:26):
in disease probably like this patient did. So
I'll take that teaching point away.
Awesome. Kaleel, what about you?
My teaching point is that high resolution CT
scan remains the initial standard to diagnose HP
like you guys highlighted prior.
And we now use less lung biopsy to
(37:46):
establish the diagnosis of HP.
Great. And, Sabia?
I think and I I'd bring it back
to the very beginning. I think that a
very good his history. I always tell my
fellows, like, concentrate on the history. The patient
will give you his diagnosis or her diagnosis.
So I think that this idea that he
(38:08):
had ongoing symptoms,
the fact that they had the mold exposure,
that hypersensitivity
in humanitis just in the very beginning would
have been higher higher in my differential.
And I think we don't emphasize it enough,
like, really hone down, get exposure
history, be really meticulous
about those kinds of things is really important
(38:29):
in taking care of your patients.
Yeah. Absolutely. Yeah. If patient told you what
he had right away, I have black mold
in my apartment. I love that.
All right. Thank you both so much for
joining us. We love doing these episodes. Thank
you all for listening in. Make sure that
you like and review wherever you're listening to
your podcast and tune in two weeks for
our next episode.
This episode was written, produced, edited by myself
(38:49):
and Christina Montemayor and music's original music by
Eric Rogers. And we'll see you next time.
See you next time. Thank you. Thanks.
Popular Podcasts
Stuff You Should Know
If you've ever wanted to know about champagne, satanism, the Stonewall Uprising, chaos theory, LSD, El Nino, true crime and Rosa Parks, then look no further. Josh and Chuck have you covered.
Dateline NBC
Current and classic episodes, featuring compelling true-crime mysteries, powerful documentaries and in-depth investigations. Follow now to get the latest episodes of Dateline NBC completely free, or subscribe to Dateline Premium for ad-free listening and exclusive bonus content: DatelinePremium.com
The Burden
The Burden is a documentary series that takes listeners into the hidden places where justice is done (and undone). It dives deep into the lives of heroes and villains. And it focuses a spotlight on those who triumph even when the odds are against them. Season 5 - The Burden: Death & Deceit in Alliance On April Fools Day 1999, 26-year-old Yvonne Layne was found murdered in her Alliance, Ohio home. David Thorne, her ex-boyfriend and father of one of her children, was instantly a suspect. Another young man admitted to the murder, and David breathed a sigh of relief, until the confessed murderer fingered David; “He paid me to do it.” David was sentenced to life without parole. Two decades later, Pulitzer winner and podcast host, Maggie Freleng (Bone Valley Season 3: Graves County, Wrongful Conviction, Suave) launched a “live” investigation into David's conviction alongside Jason Baldwin (himself wrongfully convicted as a member of the West Memphis Three). Maggie had come to believe that the entire investigation of David was botched by the tiny local police department, or worse, covered up the real killer. Was Maggie correct? Was David’s claim of innocence credible? In Death and Deceit in Alliance, Maggie recounts the case that launched her career, and ultimately, “broke” her.” The results will shock the listener and reduce Maggie to tears and self-doubt. This is not your typical wrongful conviction story. In fact, it turns the genre on its head. It asks the question: What if our champions are foolish? Season 4 - The Burden: Get the Money and Run “Trying to murder my father, this was the thing that put me on the path.” That’s Joe Loya and that path was bank robbery. Bank, bank, bank, bank, bank. In season 4 of The Burden: Get the Money and Run, we hear from Joe who was once the most prolific bank robber in Southern California, and beyond. He used disguises, body doubles, proxies. He leaped over counters, grabbed the money and ran. Even as the FBI was closing in. It was a showdown between a daring bank robber, and a patient FBI agent. Joe was no ordinary bank robber. He was bright, articulate, charismatic, and driven by a dark rage that he summoned up at will. In seven episodes, Joe tells all: the what, the how… and the why. Including why he tried to murder his father. Season 3 - The Burden: Avenger Miriam Lewin is one of Argentina’s leading journalists today. At 19 years old, she was kidnapped off the streets of Buenos Aires for her political activism and thrown into a concentration camp. Thousands of her fellow inmates were executed, tossed alive from a cargo plane into the ocean. Miriam, along with a handful of others, will survive the camp. Then as a journalist, she will wage a decades long campaign to bring her tormentors to justice. Avenger is about one woman’s triumphant battle against unbelievable odds to survive torture, claim justice for the crimes done against her and others like her, and change the future of her country. Season 2 - The Burden: Empire on Blood Empire on Blood is set in the Bronx, NY, in the early 90s, when two young drug dealers ruled an intersection known as “The Corner on Blood.” The boss, Calvin Buari, lived large. He and a protege swore they would build an empire on blood. Then the relationship frayed and the protege accused Calvin of a double homicide which he claimed he didn’t do. But did he? Award-winning journalist Steve Fishman spent seven years to answer that question. This is the story of one man’s last chance to overturn his life sentence. He may prevail, but someone’s gotta pay. The Burden: Empire on Blood is the director’s cut of the true crime classic which reached #1 on the charts when it was first released half a dozen years ago. Season 1 - The Burden In the 1990s, Detective Louis N. Scarcella was legendary. In a city overrun by violent crime, he cracked the toughest cases and put away the worst criminals. “The Hulk” was his nickname. Then the story changed. Scarcella ran into a group of convicted murderers who all say they are innocent. They turned themselves into jailhouse-lawyers and in prison founded a lway firm. When they realized Scarcella helped put many of them away, they set their sights on taking him down. And with the help of a NY Times reporter they have a chance. For years, Scarcella insisted he did nothing wrong. But that’s all he’d say. Until we tracked Scarcella to a sauna in a Russian bathhouse, where he started to talk..and talk and talk. “The guilty have gone free,” he whispered. And then agreed to take us into the belly of the beast. Welcome to The Burden.